

By Nicholas IBEKWE
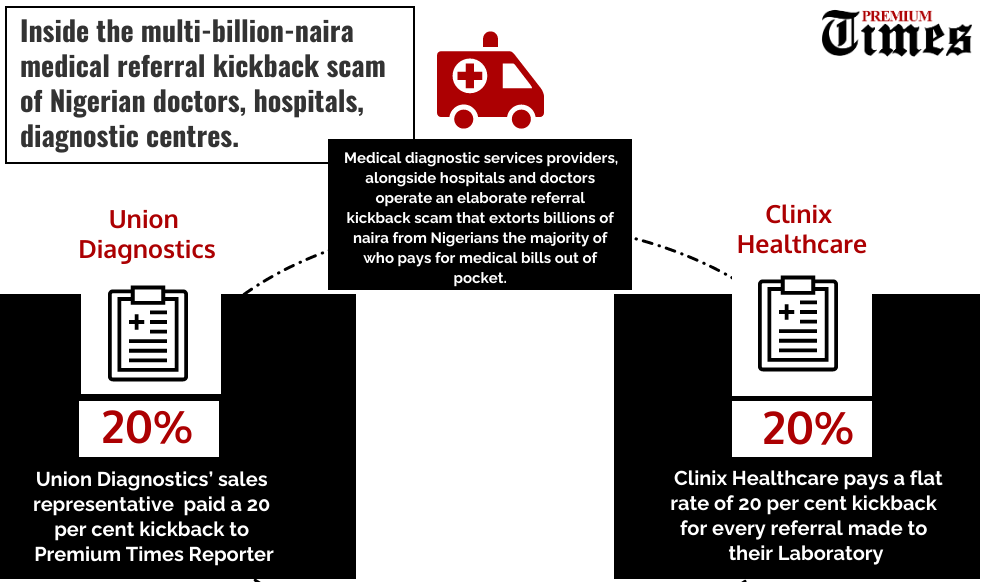
MEDICAL referral kickback is a leading cause of why a majority of Nigerians who pay for medical bills out of pocket are increasingly finding it difficult affording treatment for illness as well as the main cause of misdiagnosis and other medical complications, medical laboratory scientists and physicians told PREMIUM TIMES.
The experts also identified lax regulation as the reason the fraudulent referral kickback scheme has become entrenched.
Describing fee-splitting and the payment of kickbacks to doctors as “racketeering”, “criminal”, and “unethical”, the Association of Medical Laboratory Scientists of Nigeria (AMLSN), the professional association of medical laboratory practitioners in the country, told PREMIUM TIMES that the practice is not only entrenched but “one of the banes of the health sector in Nigeria”.
“Any place that relies on a referral laboratory service, you can be sure that they are doing fee-splitting,” Casimir Ifeanyi, the national publicity secretary of AMLSN told PREMIUM TIMES. “It is racketeering. It is destroying the system.”
Mr Ifeanyi added that the practice of fee-splitting ultimately affects the quality of diagnoses conducted by laboratories.
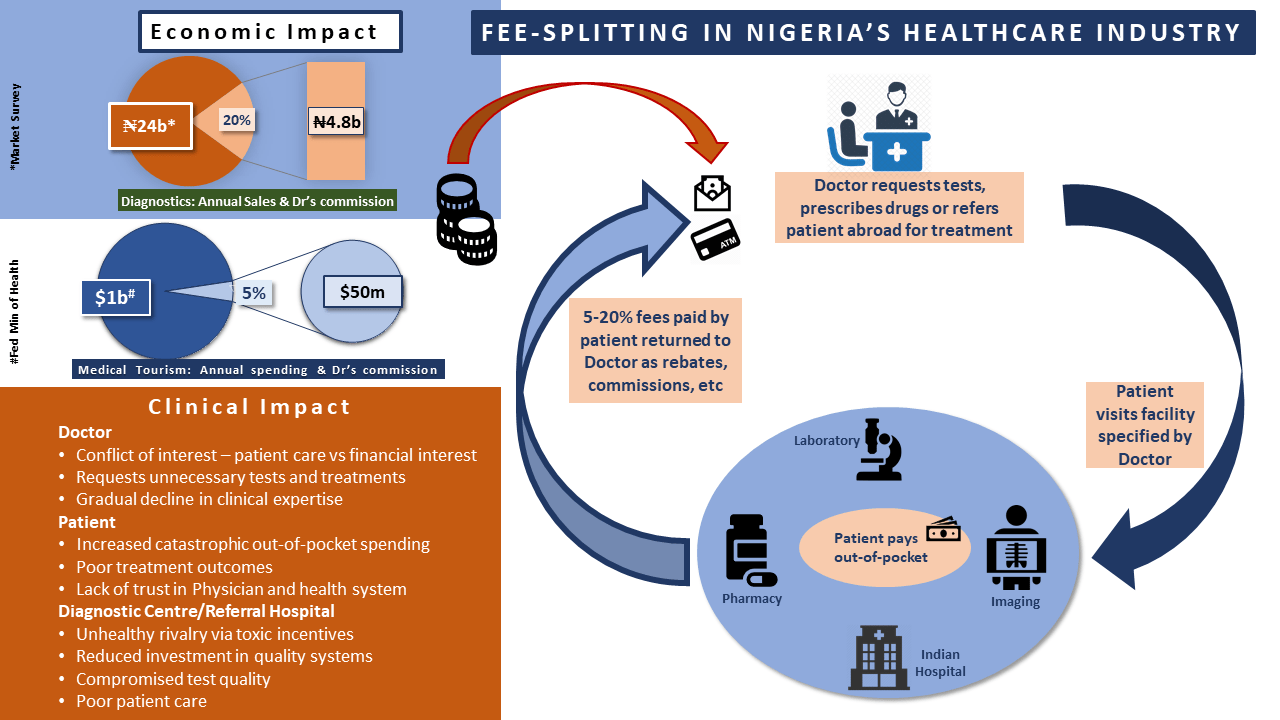
“They pay from 20 to sometimes 30 and 40 per cent,” he said. “If I have to pay that much to someone else, what will happen is that such operator will clandestinely cut corners and compromise the system because I do not see you following standard operating procedure to analyse samples using the requisite material and all the inputs and break-even so much so that you can part with up to 35 per cent.”
Medical misdiagnosis is one of the leading causes of deaths in the country. In a 2018 publication, a former president of AMLSN, Toyosi Raheem, told the Nation newspaper that misdiagnosis results in administering the wrong treatment on patients and prolong hospital stay.
“It may also cause further damage, prolonged hospital stay, unnecessary financial burden and may cause death. This will also lead to relative poor rating of Nigerian healthcare services when compared to other countries of the world,” he reportedly told the newspaper.
Mr Raheem blamed the incidence of misdiagnosis in the country on the use of substandard reagent and equipment by medical laboratory services providers, and on regulatory failure.
“Fake or substandard medical diagnostic devices/equipment and their accessories find their ways into the Nigerian market through the porous Nigerian borders. Inadequate regulatory activities of health regulatory bodies e.g. Medical and Dental Council of Nigeria, Medical Laboratory Science Council of Nigeria, Nursing and Midwifery Council of Nigeria etc.
“These health regulatory bodies statutorily regulate the activities, equipment and work environments of the respective health professionals. When the regulatory activities of the health regulatory bodies are absent, inadequate or frustrated, medical misdiagnoses will increase and sanctions on offenders will be slowed down or impossible,” Mr Raheem said.

Paschal Achunine of Health Emergency Initiative (HEI), a not-for-profit organisation that provides medical assistance for people who are financially distressed, said this kickback arrangement does not only lead to a hike in the cost of medical diagnosis, doctors are enticed to send patients for unnecessary tests knowing that the higher the volume of the referral they make the more money that will accrue to them.
“It means that the patient potentially pays out of his pocket. Because the doctor has a cut, there are three things that would happen, the patient will pay more for that lab, there might even be some tests that are not required but in order to increase the cumulative income of the doctor he could add those tests, it is percentage based and the doctor will have more money accrued to him,” he said.
Because Nigerians don’t have recourse to the law, people feel they are helpless because the legal system is not effective.
The goldmine of the healthcare sector
Although there are no official data of the actual revenue of hospitals and diagnostic centres in the country, a group of Nigerian doctors, who are opposed to the unethical referral kickback scheme, in 2018 estimated that at least N4.8 billion naira is stolen annually from poor Nigerians, majority of who pay for medical bills out of pocket.
The doctors, who asked not to be identified because they fear they would be blacklisted by their colleagues and diagnostic centres, explained that they arrived at the estimate by computing the monthly revenue of some leading diagnostics firms in the country.
The doctors also estimated that another $50 million (being 5 per cent of the $1 billion Nigerians spend on medical tourism yearly, according to a Nigerian Ministry of Health estimate) is paid to doctors and others for referral for treatment abroad.
If one considers the large number of unregistered diagnostic centres in the country and the estimated 8.5 per cent compound annual growth rate (CAGR) of the sector, the annual amount lost to this cut arrangement is several times the value of the estimate arrived at by the doctors.
Also, the Association of Medical Laboratory Scientists of Nigeria (AMLSN), the professional body of medical laboratory practitioners in the country, said medical laboratory services are the “goldmine” of the health sector.
“If a hospital, private or public, turns in N1 billion in a year, 70 per cent of that N1 billion gross earnings are earned from laboratory testing,” Mr Ifeanyi, the spokesperson for AMLSN told PREMIUM TIMES.
He said the earnings from the pharmaceutical and hospital consulting sub-sector of the healthcare sector do not come close to what accrued from medical laboratories.
“There is no drug that you will buy, there is no consultation fee you will pay, that will be several hundred per cents the cost of rendering that service. So, the goldmine in the health sector is the medical laboratory science profession,” Mr Ifeanyi added.
Loose regulation
In spite of how entrenched this illicit practice is, the regulators who should be protecting the public seems to be doing nothing about it.
PREMIUM TIMES sent an email to the Medical Laboratory Science Council of Nigeria asking what it is doing to stop the practice but weeks after the email was sent the council neither acknowledged nor replied.
When a reporter from this newspaper visited the head office of the council in Abuja, an official of its Corporate Affairs and Public Relations unit, who refused to say her name, swore she has never heard of fee-splitting between hospitals and diagnostic centres before.
“We have not had any case of medical laboratories paying doctors since we started. It is unheard of and it is impossible for medical lab scientists to pay doctors a percentage of their fee,” she said.
When reached for comment, the Medical and Dental Council of Nigerian (MDCN) said doctors reported for such misconducts are prosecuted by its disciplinary tribunal.
It, however, added that its disciplinary tribunal only reconvened in 2019 after four years of inactivity following the Nigerian government’s dissolution of the boards of agencies and parastatals in 2015.
The council added that after it reconvened in 2019, its disciplinary tribunal has, however, prosecuted two cases of fee-splitting.
“The Tribunal has tried the concerned doctors,” Enejo Abdu, an assistant registrar in charge of professional discipline, said in an email. “One was found guilty and suspended from practising Medicine in Nigeria for six months.”
However, Mr Abdu did not reveal the identity of the doctor that was sanctioned.
Innocent Ujah, the President of the Nigerian Medical Association (NMA), said he was unaware doctors receive kickbacks from medical laboratory service providers.

But when pressed further, he suggested that there was nothing wrong with the practice and compared it with the commission earned by beer suppliers from breweries.
Mr Ujah made his shocking and ludicrous comparison despite the Nigerian Code of Medical Ethics expressly prohibiting doctors from earning commissions from referrals and other services provided.
“I am not aware of that as the NMA president,” he said. “You said anybody. So, it doesn’t have to be a doctor. If you say they claim (to be doctors), then I don’t agree with you. If you say you are a doctor and they (diagnostic centres) don’t verify, then it is their own business.
“If I am doing business with you, let’s say a carton of beer and I say if I sell to you, I need a commission, that is a commission actually. Is that not what you are saying? And it is not about doctor’s alone, it is about anybody who refers a patient to them. There must be an understanding; an MoU,” he said.
When asked if the practice won’t ultimately lead to an increase in the cost of diagnosis, Mr Ujah initially said he was not in a position to comment but admitted that that was the case when pressed further.
Mr Ujah, however, became furious when told that the diagnostic centres that were the subject of this investigation made no attempt to verify if this reporter, posing as a doctor, was indeed a doctor.
“You went as a private doctor and was not identified by anybody? Then that person is a fool. That shows how porous Nigeria is. That means anybody who goes anywhere and says ‘I am a doctor’ people do not bother. That is why many people are being killed anyhow. If you come to me and say you are a doctor, you must show evidence that you are a doctor before I will talk to you. The greed in us as people. That means our patients are not protected,” he said.
But while Nigerian regulators snore away, ethical watchdogs elsewhere are wielding the big stick against doctors and laboratories involved in fraudulent practices.
In 2014, Nigerian-born Chikezie Onyenso, a certified paediatrician was sentenced to 20 months “in prison for soliciting and taking cash and rental payments as kickbacks for his patients’ diagnostic testing referrals, the United States Department of Justice announced in a statement.
“Onyenso was a licensed and board-certified paediatrician and internist who owned his own medical practice, Total Support Medical Group, in Irvington, N.J. From the summer of 2010 through December 2011 he conspired to take illegal kickbacks in exchange for sending his patients to Orange MRI. Onyenso sought and accepted thousands of dollars of cash in envelopes in exchange for referring his Medicare and Medicaid patients to Orange MRI for MRIs and CAT scans. For his ultrasound referrals, Onyenso received from Orange MRI more than $25,000 in kickback payments disguised as rental payments and documented by a bogus, $1,000-per-square-foot lease. He was recorded taking cash kickbacks in his Irvington office on Oct. 11, 2011, and Nov. 22, 2011,” the statement stated.
The judge ordered Mr Onyenso to pay a fine of $40,000 and ordered him to forfeit $42,176.
Similarly, Ashokkumar Babaria, an Indian American radiologist was sentenced to 46 months in prison for a referral scam and ordered to forfeit $2 million.
Not done in Patients’ best interest
Ike Anya, a London-based doctor, said the practice of paying kickbacks to doctors for referrals is not a recent occurrence. He said the practice was very much in play in the 1990s when he was a young doctor in Nigeria.
Dr Anya, who also teaches Ethics at the London School of Hygiene and Tropical Medicine (LSHTM), said the practice is one hitting at the core of medical ethics.

“If a doctor is benefitting from a referral how are the patients convinced that the referral is in their own best interest and not motivated by the doctor’s benefits. There is no way of telling that,” he said.
“That is why medical ethics states that you are always making decisions in the patient’s best interest and not any other considerations and certainly not for financial benefits to yourself.”
Dr Anya said although the practice of paying and collecting kickbacks in the health industry is not unique to Nigeria, in other places where it occurs, regulators are quick to put it in check, unlike Nigeria.
“It has been shown to happen even in the US and in the UK in various forms – private hospitals having some form of formal arrangements where they try to steer patients towards each other,” he said. The challenge, particularly in Nigeria, is where is the regulator in all of these?”
He said in a situation where the statutory regulator in Nigeria was without a board for four years makes regulation even more porous. He said doctors and other medical practitioners need constant reminders of the ethics of their professions.
He also said campaigns to enlighten the public about possible unethical practices and their rights may help to dissuade some medical practitioners from indulging in unethical practices.
“There is the question of the educators of doctors and medical laboratory scientists. Medical ethics is something that is not emphasis much in our training in Nigeria,” Dr Anya added.
“In terms of solutions, regulators need to up their game. There is a need for constant education about ethics to doctors and medical practitioners.
“Public awareness but what is the patient going to do? When a patient is going to the doctor there is what the economists call asymmetry of information. The doctor is the one who knows what tests you need. It is the doctor that knows that. And if they say to you go to this lab, you are not in a position to say I don’t want to go to that lab.
“Also, when you are ill, it automatically puts you in a vulnerable position, no matter how powerful or how rich you are when you are ill, you just want to get better. You just want to do whatever it is to get better.
“In spite of that, there should be public awareness and campaign to tell patients that this is what is going on, maybe if more patients start asking questions, it might turn some people to stop.”
We will investigate laboratories if presented with evidence of wrongdoing – Consumer Agency
The Federal Competition and Consumer Protection Commission (FCCPC) said it is neither aware of the rebate arrangement between diagnostic centres and doctor nor has it received any complaint of that nature.
It, however, vowed to intervene, using the appropriate legislations, if presented with evidence of such unethical practices.
“A key and flagship initiative of the FCCPC is the Patients Bill of Rights (PBoR), which requires transparency in billing and full disclosure of necessary procedures and cost of such procedures by the relevant facility. As such, under the PBoR, this would be wrong,” the director-general of the commission, Tunde Irukera, told PREMIUM TIMES.
“In addition, S.17(g) and (s) prohibit unfair, unconscionable, obnoxious and deceptive marketing, trading and business practices as well as unscrupulous exploitation of consumers.
“With respect to direct provisions on pricing S.115, 127 prohibit unclear and well as unreasonable or manifestly unjust pricing (gouging or profiteering), while S.124 prohibits unfair dealings such as using unfair tactics to take advantage of consumers, or anyone’s vulnerability.
“With the combination of these provisions, if the FCCPC has probable cause or receives credible allegations or intelligence, the Commission will certainly proceed to open an investigation into the operations of the target of the investigation, and to the extent that evidence leads further, broaden the investigation to address an expanded scope if it’s an industry-wide practice.
“In addition, the FCCPC will coordinate and collaborate with the relevant professional disciplinary regulator and provide the outcome of its investigation to see any professional disciplinary action required, where applicable,” he said.

He said the outcome of its investigation and consequences will result in “a behavioural modification and a regulatory tool that prevents continuing abuse.”
Mr Irukera also said consumer education about the existence of the practice will help in addressing it.
“Further, consumer education about the existence of such a problem, and advice to consumers about their rights in the circumstances will assist in addressing the problem. Finally, engagement and advocacy with the relevant trade or professional associations about enforcing their ethics or other behavioural codes will be helpful,” he said.
CLICK HERE TO READ THE FIRST PART OF THIS STORY.
This report is published with permission from Premiumtimesng.com