

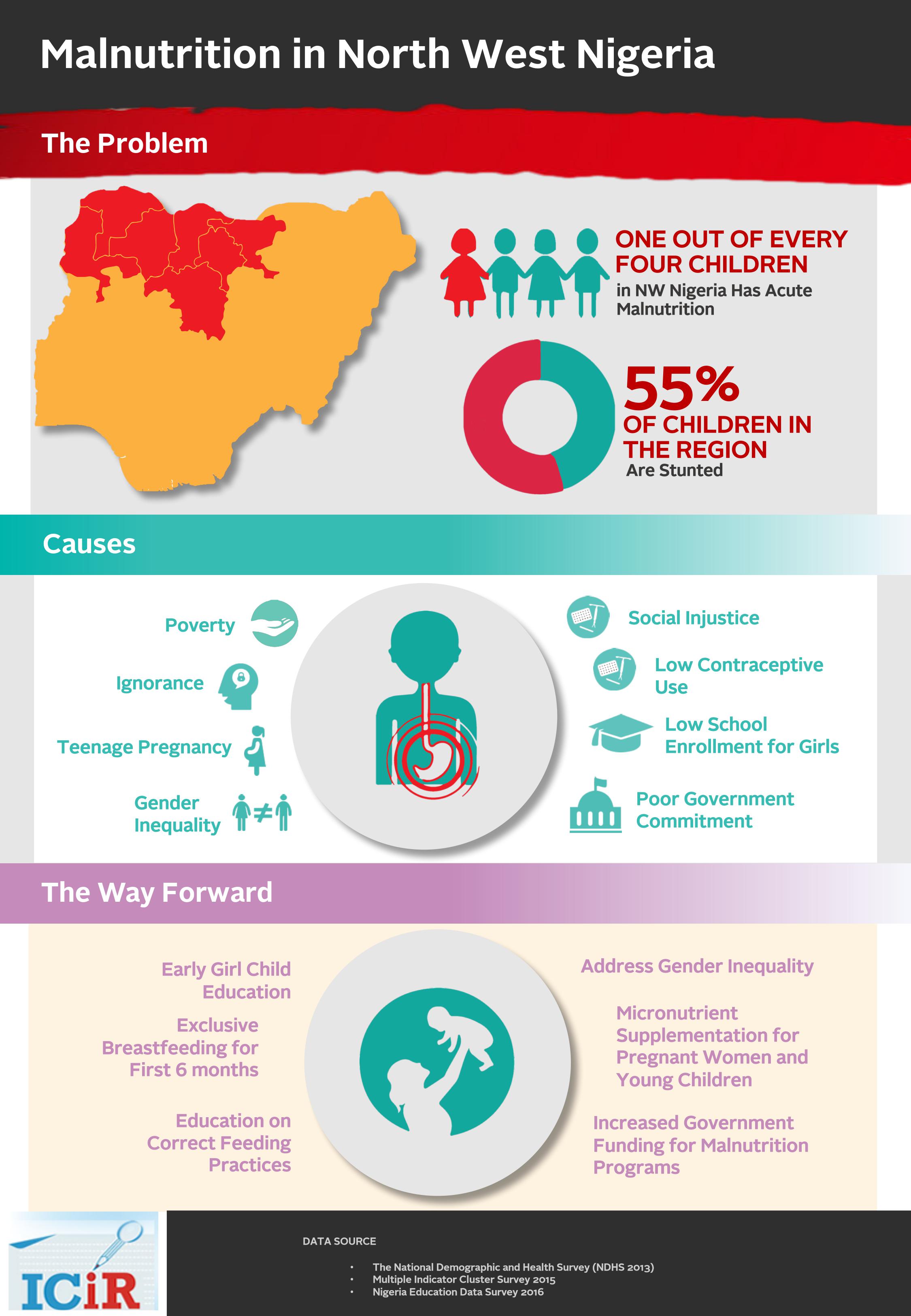
North West, the most populated region in Nigeria, has the highest undernourished children. Fifty-five percent of children in the region are stunted, suggesting they are not growing proper physically or mentally. The region is not affected by the Boko Haram conflict, yet one out of every four children has acute malnutrition. Health facilities are overwhelmed by malnourished children, many of whom do not survive beyond their fifth birthday. In this first of two-part series, CHIKEZIE OMEJE reports that the causes of this silent crisis of malnutrition are not just hunger and poor knowledge of nutritious foods. Rather, the region’s problem stems from deeply rooted gender inequality and social injustice.
Fatima spoon-feeds her two-year-old son, Bashir Kamilu, with Kwashi pap for breakfast. Moments after eating, he excretes it in loose stool, seeping through his oversize diaper. Fatima lets the stream of watery faeces drop on a sheet she has spread beneath his buttock on the hospital bed.
Kwashi is a polite and short-term that health workers have adopted for Kwashiorkor, a severe protein-energy deficiency that Kamilu began to suffer after Fatima weaned him from breast milk and put him on a diet high in carbohydrates.
Kwashiorkor was a commonly-used word in Nigeria about 50 years ago during the Biafra-Nigeria Civil War, when about a million children died of malnutrition in the eastern region. Pictures of the 30-month war showed starving children with emaciated bodies or bloated stomachs.
Almost five decades after the war, similar pictures of malnourished children are creeping in from every part of the country, but have assumed a darker dimension in the North West.
The region is breeding undernourished children. A half of the children are stunted and one out of every four children has acute malnutrition.
“More than 80 percent of the children we see in this hospital are malnourished,” says Salma Suwaid, the head of paediatric ward at Muhammadu Abdullahi Wase Specialist Hospital, Kano. “It’s consuming the system.”
Each morning, Kwashi pap is brought to Kamilu and more than 20 other children in the hospital. The pap, which contains millet, suya beans, groundnut, palm oil and crayfish, is supplied by the nutritional unit of the hospital. It is meant for families who cannot afford packaged – and usually imported – nutritional supplements.
Malnourished children have weak immunity which makes them vulnerable to infectious diseases.
Kamilu suffers diarrhoea and he has a cough and skin infection. When ICIR met him, he had been admitted to the hospital eight days earlier. After the diarrhoea started, Fatima had given him local herbs. She later took him to a local drug store, which gave him medicine. The diarrhoea persisted, and eventually, the cough and skin infection took hold. Fatima obtained the consent of her spouse to take Kamilu to the hospital where he was diagnosed with severe acute malnutrition.

Severe acute malnutrition is the most extreme and visible form of undernutrition. Children who have this condition are frail and skeletal. They have very low weight relative to their height and severe muscle wasting. They may also have nutritional oedema – characterized by swollen feet, face and limbs.
Undernutrition is indicated in three ways: “Stunting,” which occurs when a child’s height is low for his or her age; “underweight,” when the weight is low for the age; or “wasting,” which is when the weight is not proportionate to the height.
Here in the hospital, Fatima sits beside Kamilu on the bed and replenishes the lost pap with Awara, a local suya beans cake. When he coughs, tiny Awara with saliva flows out of his mouth. He is in a daze, struggling to eat the Awara that his mother is stuffing into his mouth. His ribs are visible, and the skin on his fingers and feet is peeling off.
“I was giving him Tuwo and other foods in the house,” says Fatima in Hausa.
At 25, she has given birth five times but has four surviving children. Married at 17, she is a second wife to the man who has come to the hospital just twice since Kamilu was admitted.
WHY ARE THEY BECOMING MALNOURISHED?

Health workers often attribute malnutrition in North West to poverty, noting that at times parents are simply too poor to afford nutritious foods. But even when they can pay to give their children better diets, some people have too little knowledge to do so.
“Our normal culture here is that you give them pap,” Kabiru Ibrahim, the Executive Secretary of Jigawa State Primary Health Care Development Agency told the ICIR. “The pap has no nutrients whatsoever. A child who continues to take the pap will become wasted.”
Children also are improperly weaned from breastfeeding, he adds. “One day, the mother will decide to wean the child off breast milk and the child will be taken to the grandmother several villages away from the mother. The child who had been fed just breast milk up to that morning no longer gets breast milk but only pap. Children cannot cope.”
But to say that young children are not fed properly misses a deeper truth. The underlying problem is that many women never get the opportunity to learn how to feed their children. Often, entitled polygamous men marry underage girls, impregnate them and keep them in seclusion, never caring for the many children they produce.
In Kano and other cities in the North West, hundreds of thousands of the boys born this way end up roaming the streets, begging for alms in tattered clothes and often without footwear. The girls are married off at teenage, continuing the cycle.
On the day ICIR visited Muhammadu Abdullahi Wase Specialist Hospital, a teenage mother, Aisha Murtala, gathered her son on her lap while sitting on a chair in the consultation room at the emergency section. Her son had been diagnosed with severe acute malnutrition and would require admission to the hospital.
Murtala, a second wife, did not have her spouse’s permission to stay in the hospital. So she had to go back home to seek his consent and obtain money from him. Since she got married, she had been kept in Purdah and was not allowed to go anywhere without the husband’s permission.
Before the son turned six months, Murtala had started giving him water, and later pap.
“Whenever the weather became very hot, I often gave him water because he would be thirsty,” says Murtala in Hausa.
A lot of teenage mothers in the region are naïve about child care. This is why malnutrition is common among the children of underage mothers.
Salma Suwaid, the head of paediatric ward in the hospital, told the ICIR that malnourished children either come from teenage mothers or women with a lot of children and inadequate resources to take care of them.
“The younger the mother is, the more likely the child will be malnourished because she is naïve about child caring. If a 12 to 13-year-old is having a child, that’s a big problem because she hasn’t finished knowing about herself, let alone taking care of a child.”
The National Demographic and Health Survey (NDHS 2013) indicates that almost a half of women in the North West have their first child when they are still adolescent.
If Murtala eventually obtains the consent of her spouse for her son’s admission, she still may not be lucky enough to secure a bed space for him. On the day ICIR visited, there was no bed space to admit children who were being diagnosed with severe acute malnutrition at the emergency section of the hospital.
In the corridor of the emergency section of the hospital, Bilkisu Sadik watches over her six-year son, Abdullahi, who lies on her wrapper on the floor with a cable that extends from his nose to an oxygen machine. Another cable extends from the oxygen to an elderly man lying on the floor beside him. Sadik brought him to the hospital with a complaint of malaria but diagnosis confirms that he has severe acute malnutrition.
Sadik does not know her age, but she appears to be in her late twenties. She was a teenage bride and has had seven babies, but only five are still alive. Though she is the husband’s first wife, he has married a second wife whom he shows more attention, she says.

At the other end of the corridor is Aisha Ubah, whose hands are on her cheeks, looking after her five-year-old son, Hamidu, who is placed on a bed. He was having a headache and shaking when Ubah brought him, her sixth child, into the hospital, but diagnosis confirms that he too has severe acute malnutrition.
The hospital emergency is crowded with mothers and their children who are mostly suffering from malnutrition. From the emergency room to the paediatric ward, women and their sick children are sleeping on mats they spread on the floor.
An average woman in the North West will have five births under the age of 27. Only 1 percent of women aged 15-49 use any method of family planning in the North Western states of Jigawa, Kano, Katsina, Kebbi, and Sokoto. Overall, only 4.3 percent of the women of reproductive age use any method of contraception in the region.
Health workers say the high birth rate increases the risk of malnutrition. Most of the women stop breastfeeding when they realise that they have become pregnant.
When the girls are married, they are denied education. Most are married to older men who already have wives. The women are subjected to Purdah. They do not earn income and they depend on whatever foods that the spouses provide.
Girls’ school enrolment in the North West is still less than 50 percent. Uneducated women are more likely to have undernourished children and bear large numbers of children.
On the day that ICIR visited Yan’Awaki Primary Health Centre along the IBB Road in Kano where hundreds of women bring their malnourished children to receive nutritional supplements, none of the women attended secondary school. They neither understand nor speak English, which is the language of instruction in schools.
A LOW PRIORITY FOR GOVERNMENT

Unicef, the UN children’s agency, introduced Community-based Management of Acute Malnutrition (CMAM), a pilot programme in Gombe State in 2009. The programme was later extended to 12 other states in the north.
Under CMAM, malnourished children who are six months to five years are given Ready-to-Use Therapeutic Food (RUTF) for about two months. The RUTF is a peanut-based paste, which contains milk powder, sugar and multiple micronutrients.
More than two million children with severe acute malnutrition have been rehabilitated since this programme began, according to Unicef.
Currently, an estimated 2.5 million Nigerian children under five have severe acute malnutrition. To survive, they need urgent treatment.
Unicef puts the cost of treating a malnourished child under the CMAM at N50, 000. To cover all the affected children in the country, it would cost about N95 billion.
For the first time since Unicef began the programme in the selected states, the Federal Government provided N1.2 billion in the 2017 budget to purchase RUTF. This is a substantial improvement considering that only N2 million was budgeted for nutrition in 2016, and the money was never released.
CMAM has largely been financed by the British charity, the Children’s Investment Fund Foundation (CIFF) with counterpart funding from the states that are benefitting from the programme.
However, the continuation of CMAM is threatened by the inability of the states to meet its financial obligations.
Kano State is expected to contribute N320 million out of the N826 million for the implementation of CMAM in the state this year. But as at last month, just two months to the end of the year, the state has not made this contribution.
Ibrahim Maryam, the acting chairman of Partnership for Advocacy in Child and Family Health (PACFAH) in Kano State told the ICIR that the government is not committed because decision-makers are not affected by malnutrition.
“They don’t see this kind of problem in their homes, and they are far away from the rural communities who are the major victims,” says Maryam.
“Can you imagine an organisation like Unicef will be giving higher support to fight malnutrition while the government is not even paying its counterpart funding?
“Then the programme will stop and we will come back to zero. Those already on treatment will deteriorate and die.”
The state is already facing a stock out of RUTF. Last month, Yan’Awaki Primary Health Centre along the IBB Road in Kano suspended the admission of malnourished children into the CMAM programme.
Bilkisu Waziri who is in charge of the programme at the health centre told the ICIR that they decided to stop admitting new patients so that the remaining stock of RUTF will cover the children who are already receiving treatment. But even at that, the quantity being given to the children has been slashed by a half. Those who used to get 14 pieces are being offered seven pieces. A child is fed two sachets of RUTF per day.
“We only have 14 cartons left and we have more than 300 children to cover today,” says Waziri. Each carton of RUTF contains 150 pieces.
On Thursdays, when mothers bring their children to receive their RUFT, Waziri says they attend to about 500 hundred malnourished children. The health centre is one of the 30 CMAM centres in six local government areas in the state.
Some health workers allege that Unicef has stopped supplying the imported RUTF because the government refused to pay its counterpart fund.
Halima Yakassai, the Kano State Nutrition Officer, says the state has not stopped the programme, adding that it is making arrangements to launch a new version of RUTF to be branded with logos of Kano State Government and Unicef.
She points out that she has just received a new supply of about 6,000 cartons from Unicef which she will start the distribution very soon.
However, Auwal Mohammed, a member of the Civil Society for Scaling Up Nutrition (CS-SUN) in Kano State told the ICIR that tackling malnutrition in the region requires addressing inequality of women and addressing the social issues have that created worsening conditions for children.
Mohammed says the men who marry young girls do not provide adequate nutritious foods for the women and children.
He argues that the RUTF programme is not sustainable because the number of malnourished children keeps increasing.
“RUTF is helpful,” says Mohammed. “Even though it’s not a sustainable solution, those who are malnourished need to be remedied.
“The women have to be educated. Instead of getting married, they should be sent to school.”
According to Unicef, steps to prevent children becoming malnourished include supporting and encouraging mothers to breastfeed their babies exclusively for the first six months of life; educating families about the correct feeding practices for older babies and children; and providing micronutrient supplements and vitamins and fortified food for pregnant women and young children.
Fatima Maiyalli, a public health nurse and former coordinator of child health in Kano State’s ministry of health, told the ICIR that massive education is needed to reverse the trend of malnutrition in the North West because there is so much ignorance
“Our men believe that family affairs are just for the women,” says Maiyalli. “If the men can support their wives in providing care to the children, it will solve most of the problems of malnutrition.”
This report was made possible by Early Childhood Development Reporting Fellowship, a project by the International Center for Journalists (ICFJ).
Chikezie can be reached at comeje@icirnigeria.org. Follow him on Twitter: @KezieOmeje